
Left Ventricular Geometry and Left Ventricular Hypertrophy Phenotype in Newly Diagnosed Hypertension in North-eastern Nigeria
Main Article Content
Keywords
Left Ventricular Hypertrophy, Hypertensive Heart Disease, Left Ventricular remodelling, Left Ventricular Geometry.
Abstract
Background: Left Ventricular Hypertrophy (LVH) is a key component of hypertensive heart disease. The prevalence of hypertensive LVH ranges from 19% to 48 % in untreated hypertensive patients amongst the Western population but is 46% to 63% in Nigeria. The study aims to highlight the prevalence of LVH and to determine the pattern of LV geometry and the LVH phenotype in newly diagnosed hypertensive patients.
Methodology: The study was cross-sectional, and observational between June 2019 and June 2021. The study population comprised 300 newly diagnosed hypertensive adult patients aged 18 years and above, and 300 Healthy age, sex-matched non-hypertensive adults as control groups. An echocardiography was performed and the diagnostic criteria for LVH, LV Geometry and LVH phenotype were used based on the American Society of Echocardiography and the European Association of Cardiovascular Imaging.
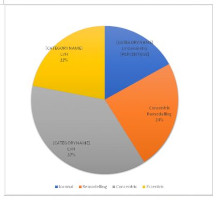
Results: The total number of study participants was 600, three hundred newly diagnosed hypertensive patients and three hundred normotensive controls. The male participants comprised 180 (60%) of the newly diagnosed hypertensive cases and 120 (40%) of the normotensive controls, while the female participants accounted for 168 (56%) of the hypertensive group and 132 (44%) of the control group, respectively. Overall, 59% of newly diagnosed hypertensive patients had LVH. Concentric LVH was the commonest LV geometry with a prevalence of 37% among newly diagnosed hypertensive patients. Fifty-five point four per cent (55.4%) of newly diagnosed hypertensive patients had concentric non-dilated hypertrophy.
Conclusion: LVH is highly prevalent and occurs in more than half of newly diagnosed hypertensive patients. The commonest LV geometry is concentric hypertrophy, and the LVH phenotype of concentric non-dilated Hypertrophy accounts for more than half of LVH.
References
2. Dumitrescu M, Constantin A, Nemecz AM, Drăgan E, Popov LD, Tanko G. Hypertension induces compensatory left ventricular hypertrophy by a mechanism involving gap junction lateralization and overexpression of CD36, PKC and MMP-2. Rom J Morphol Embryol. 2021;62(3):713–21.
3. Verdecchia P, Porcellati C, Reboldi G, Gattobigio R, Borgioni C, Pearson TA, et al. Left ventricular hypertrophy as an independent predictor of acute cerebrovascular events in essential hypertension. Circulation. 2001;104(17):2039–
44.
4. Nemtsova V, Burkard T, Vischer AS. Hypertensive Heart Disease: A Narrative Review Series—Part 2: Macrostructural and Functional Abnormalities. J Clin Med. 2023;12(17):1–18.
5. Cuspidi C, Sala C, Negri F, Mancia G, Morganti A. Prevalence of left-ventricular hypertrophy in hypertension: an updated review of echocardiographic studies. J Hum Hypertens. 2012 Jun 24;26(6):343–9.
6. Sárközy M, Gáspár R, Zvara Á, Siska A, Kővári B, Szűcs G, et al. Chronic kidney disease induces left ventricular overexpression of the pro-hypertrophic microRNA-212. Sci Rep. 2019;9(1):1–16.
7. Karaye K., Habib A. Pattern of left ventricular geometry in hypertension: a study of a hypertensive population in
Nigeria. Sahel Med J. 2010 Jul 1;12(4).
8. Adamu UG, Kolo PM, Katibi IA, Opadijo GO, Omotosho ABO, Araoye MA. Relationship between left ventricular diastolic function and geometric patterns in Nigerians with newly diagnosed systemic hypertension. Cardiovasc J Afr. 2009;20(3):173–7.
9. Aje A, Adebiyi AA, Oladapo OO, Dada A, Ogah OS, Ojji DB, et al. Left ventricular geometric patterns in newly presenting Nigerian hypertensives: An echocardiographic study. BMC Cardiovasc Disord. 2006;6(Lv):1–6.
10. Ganau A, Devereux RB, Roman MJ, De Simone GS, Pickering TG, Saba PS, et al. STUDIES IN HYPERTENSION Patterns of Left Ventricular Hypertrophy and Geometric Remodeling In Essential Hypertension. 1550;19(7):1550–8.
11. Abdalla M, Booth JN, Diaz KM, Sims M, Muntner P, Shimbo D. Hypertension and alterations in left ventricular structure and geometry in African Americans: the Jackson Heart Study. J Am Soc Hypertens. 2016 Jul;10(7):550-558.e10.
12. Nogueira JB. Left ventricular hypertrophy in systemic hypertension. Benefits of its reversal. Arq Bras Cardiol. 1999 Jul;73(1):108–12.
13. Khouri MG, Peshock RM, Ayers CR, de Lemos JA, Drazner MH. A 4-Tiered Classification of Left Ventricular Hypertrophy Based on Left Ventricular Geometry. Circ Cardiovasc Imaging. 2010 Mar;3(2):164–71.
14. Brees AJ, Pluim BM, Vliegen HW, de Roos A, Lamb HJ, van der Wall EE. Assessment of Left Ventricular Hypertrophy: A Comparison of Electrocardiography, Echocardiography and Magnetic Resonance Imaging. In: Left Ventricular Hypertrophy Physiology versus Pathology. 1999. p. 43–53.
15. Mohan G, Kaur R, Kamra A, Aggarwal A. A Comparative Study of Electrocardiographic and Echocardiographic Evidence of Left ventricular Hypertrophy. AMEI’s Curr Trends Diagnosis Treat. 2017 Dec;1(2):59–63.
16. Galtimari IA, Faruk B, Imhoagene-Albert O, Talle MA, Anjorin CO. Prevalence of Aortic Root Dilation and Correlates of Aortic Root Dimensions in Treatment Naïve Hypertensive Patients in North-Eastern Nigeria. Niger Med J. 2023;64(2):227–42.
17. Devereux RB, Reichek N. Echocardiographic determination of left ventricular mass in man. Anatomic validation of the method. Circulation. 1977 Apr;55(4):613–8.
18. Lang RM, Badano LP, Mor-Avi V, Afilalo J, Armstrong A, Ernande L, et al. Recommendations for Cardiac Chamber Quantification by Echocardiography in Adults: An Update from the American Society of Echocardiography and the
European Association of Cardiovascular Imaging. Eur Hear J – Cardiovasc Imaging. 2015 Mar;16(3):233–71.
19. Lang RM, Bierig M, Devereux RB, Flachskampf FA, Foster E, Pellikka PA, et al. Recommendations for Chamber Quantification: A Report from the American Society of Echocardiography’s Guidelines and Standards Committee and the Chamber Quantification Writing Group, Developed in Conjunction with the European Association of Echocardiograph. J Am Soc Echocardiogr. 2005 Dec;18(12):1440–63.
20. Adekunle A, Adeseye A, Adebayo O, Olatayo A, Joseph O, Ayodele A. Left ventricular mass formulae and prevalence rates of echocardiographic left ventricular hypertrophy in Nigerians with essential hypertension. N Am J Med Sci. 2013;5(5):325.
21. Salako BL, Ogah OS, Adebiyi AA, Adedapo KS, Bekibele CO, Oluleye TS, et al. Unexpectedly high prevalence of target-organ damage in newly diagnosed Nigerians with hypertension. Cardiovasc J Afr. 2007;18(2):77–83.
22. Cuspidi C, Facchetti R, Bombelli M, Tadic M, Sala C, Grassi G, et al. High normal blood pressure and left ventricular hypertrophy echocardiographic findings from the PAMELA population. Hypertension. 2019;73(3):612–9.
23. Verdecchia P, Schillaci G, Borgioni C, Ciucci A, Gattobigio R, Zampi I, et al. Prognostic value of left ventricular mass and geometry in systemic hypertension with left ventricular hypertrophy. Am J Cardiol. 1996 Jul;78(2):197–202.
Article Sidebar
Article Details

This work is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International License.
This is an open-access journal and articles are distributed under the terms of the Creative Commons Attribution Non-Commercial Share-Alike License 4.0. This licence allows users to download and share, remix, tweak and build upon the article for non-commercial purposes, so long as the original authorship is acknowledged and the new creations are licensed under identical terms.
Ibrahim Abubakar Galtimari, Cardiology Unit, Department of Internal Medicine, University of Maiduguri Teaching Hospital, Nigeria.
Department of Medicine, Faculty of Clinical Sciences, College of Medical Sciences, University of Maiduguri, Nigeria.
Chiroma Ijuptil, Endocrinology Unit, Department of Medicine, Internal Medicine, University of Maiduguri Teaching Hospital, Nigeria
Department of Medicine, Faculty of Clinical Sciences, College of Medical Sciences, University of Maiduguri, Nigeria
Sulaiman Mohammad Maina, Department of Medicine, Faculty of Clinical Sciences, College of Medical Sciences, University of Maiduguri, Nigeria.
Nephrology Unit, Department of Internal Medicine, University of Maiduguri Teaching Hospital, Nigeria
Faruk Buba, Cardiology Unit, Department of Internal Medicine, University of Maiduguri Teaching Hospital, Nigeria.
Department of Medicine, Faculty of Clinical Sciences, College of Medical Sciences, University of Maiduguri, Nigeria.
Mohammed Abdullahi Talle, Cardiology Unit, Department of Medicine, University of Maiduguri Teaching Hospital, Nigeria. Department of Medicine, Faculty of Clinical Sciences, College of Medical Sciences, University of Maiduguri, Nigeria.
Department of Medicine, Faculty of Clinical Sciences, College of Medical Sciences, University of Maiduguri, Nigeria.