
A Case of Frequent Blinking and Abnormal Eyeball Movement Associated with Generalized Epilepsy https://doi.org/10.60787/NMJ-63-6-143
Main Article Content
Keywords
frequent blinking, abnormal eye movement, jerky leg movement, generalised epilepsy, frontotemporal dominance, sodium valproate, eyelid myoclonus
Abstract
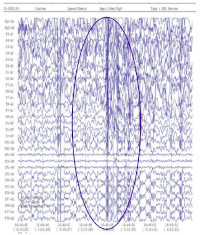
Eyelid myoclonus is an idiopathic generalized epileptic syndrome that can occur with or without absence seizures. The features include frequent blinking, an upward roll of the eyeballs, and slight backward movement of the head. It can be spontaneous or stimulated by light. Light and eyelid closure are triggers to the seizures. A 13-year-old young male student presented with a four months history of frequent blinking and abnormal eye movements. There was a positive history of leg tapping while asleep which started a year prior to presentation, but there was no loss of consciousness. On presentation, the patient was a young healthy looking myope who frequently blinks with sudden upward and left jerky movements of the eyeballs. Visual acuity was CF at 2 meters in both eyes improving with -4.50DS to 6/6. Intraocular pressures were 12 mmHg bilaterally. Anterior and posterior segment findings were normal. Brain MRI was normal, but EEG was abnormal with features suggestive of generalized epilepsy. He was co-managed with the neurologist and placed initially on Tabs Sodium valproate 250mg for 3 months. This was modified to Tabs Sodium Valproate (controlled release) 500mg at night since there was little change. This resulted in an appreciable reduction in blinking and abnormal eye movement. The leg tapping stopped on this dose. Eyelid myoclonus (EM) is a rare form of epilepsy. It is of utmost importance to create awareness of the disease among physicians. Early diagnosis and treatment are important prognostic factors of the disease.
References
2.Fisher RS. The New Classification of Seizures by the International League againstEpilepsy 2017. Curr Neurol Neurosci Rep. 2017; 17:48. doi:10.1007/s11910-017-0758-6
3.Viravan S, Go C, Ochi A, Akiyama T, Carter Snead O 3rd, Otsubo H. Jeavons syndrome existing as occipital cortex initiating generalized epilepsy. Epilepsia. (2011) 5 2:1 273–9.doi:10.1111/j.1528-1167.2011.03068.x
4.Giraldez BG, Serratosa JM. Jeavons syndrome as an occipital cortex initiated generalizedEpilepsy: further evidence from a patient with aPhotic-induced occipital seizure.Seizure.2 0 1 5; 32:7 2 – 4.d o i: 10.1016/j.seizure.2015.09.003
5.Yetman D and York-Morris S. Identifying and Treating Nocturnal Seizures, Epilepsy and seizures during sleep [Internet] Healthline Media a Red Ventures Company; [Updated 2021/12/7 ;cited 2022/7/9]. Available from https://www.healthline.com/health/epilepsy/nOcturnal-seizures.
6.Uchida C, de Carvalho KC, Guaranha M, Guilhoto L, de Araujo FG, Yacubian E. Prognosis of juvenile myoclonic epilepsy with eye-closure sensitivity. Seizure. (2018) 62:17–25. doi: 10.1016/j.seizure. 2018.09.006
7.Wang XL, Bao JX, Liang-Shi Tie-Ma, Deng YC, Zhao G, et al. Jeavons syndrome in China. Epilepsy Behav. (2014) 32:64–71. doi: 10.1016/j.yebeh.2013.12.016
8.Covanis A, Gupta AK, Jeavons PM. Sodium valproate: monotherapy and polytherapy. Epi lepsia 1982;23:693 -720.doi:10.1111/j.1528-1157.1982.tb05085.x
9.Betjemann JP, Lowenstein DH. Status epilepticus in adults. Lancet Neurol. (2015) 1 4: 615 – 24. d o i:10.1016/S1474-4422(15)00042-3
10.Kinsbourne M. Myoclonic encephalopathy of infants. J Neurol Neurosurg Psychiatry. 1962; 25:271-276
Article Sidebar
Article Details

This work is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International License.
This is an open-access journal and articles are distributed under the terms of the Creative Commons Attribution Non-Commercial Share-Alike License 4.0. This licence allows users to download and share, remix, tweak and build upon the article for non-commercial purposes, so long as the original authorship is acknowledged and the new creations are licensed under identical terms.
Adaora C Okudo, Rachel Eye Center, Abuja & Department of Ophthalmology, Asokoro District Hospital, Abuja, Nigeria
Senior Lecturer, Department of Ophthalmology, Nile University of Nigeria, Abuja, Nigeria.
Olufemi E Babalola, Rachel Eye Center, Abuja & Department of Surgery, Bingham University, New Karu, Nasarawa, Nigeria
Professor of Ophthalmology, Department of Surgery, Bingham University, NewKaru/ Jos, Nigeria.
Ifeyinwa Ani-Osheku, Department of Neurology, Asokoro District Hospital, Asokoro, Abuja, Nigeria.
Lecturer, Department of Neurology, Nile University of Nigeria, Abuja, Nigeria